




Pregnancy Must Reads

IVF Pregnancy Calendar
In vitro fertilization, or IVF is a medical procedure that has allowed struggling families conceive children. What is IVF?…

Understanding Doulas
What Are Doulas? The term “doula” originates from ancient Greek and translates to “a woman who serves”. It is…

Spotting During Pregnancy
Spotting is one of the most common concerns pertaining to pregnancy. It is estimated that around 20% of women spot…
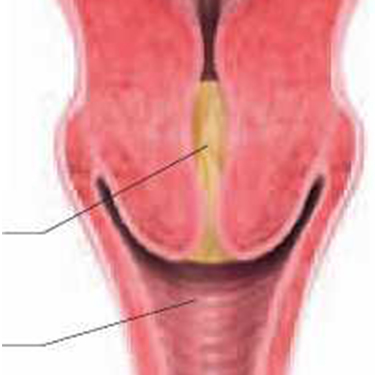
Discharging of the Mucus Plug
Many aspects of pregnancy can cause alarm to expectant mothers. One of the most alarming situations one might deal with…
Pregnancy Week 1
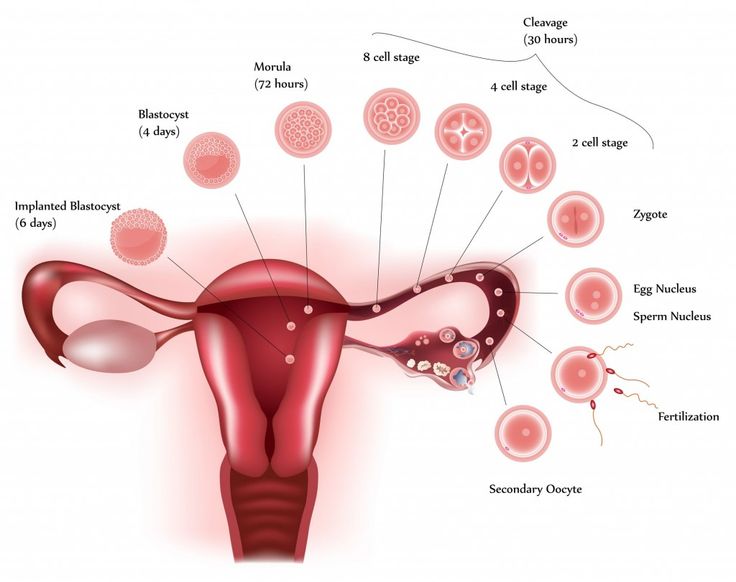
This is the very beginning of it all. At this initial stage, there is no indication that a woman is…
Pregnancy Week 2
The second week of pregnancy picks up where the first week left off. Implantation is completed in the second week…
Pregnancy Week 3
Week three is where the real fun begins. This is the first week where pregnancy symptoms could be experienced. Women…

Week 4 Pregnancy Ultrasound
Source: newhealthadvisor.com The fourth week of pregnancy is when the first visible changes occur. During week…
Week 5 Pregnancy Ultrasound
Week 5 starts with the ongoing development of the internal organs, including the central nervous system and the heart. New…

Week 6 Pregnancy Ultrasound
By the sixth week, most expectant mothers know that they are expecting. They are slowly getting used to the idea…

Week 7 Pregnancy Ultrasound
The mother’s body is changing and the baby is growing. During this week, both the uterus and the baby have…
8 Weeks Pregnant Ultrasound
What to Expect? Week 8 marks the two month period of pregnancy. Most expectant parents are excited about the news…


Pregnancy Pictures

Baby Nusery

Pregnancy Videos
